Scope of services

Nerve compression / Closed nerve injury
Nerve compressions or closed nerve injuries often present as tingling &/ numbness distal to the region of compression / injury. Few cases may also present with proximal joint involvement.
Initial management is medical and supportive with usage of anti inflammatory medicines and splintage. This usually resolves most of the lesions. If symptoms persist beyond 12 weeks microsurgical decomression with neurolysis or nerve repair ( with or without tendon transfer ) gives quick and definitive relief.
Occasional cases benefit with transposition (rerouting) of nerve.
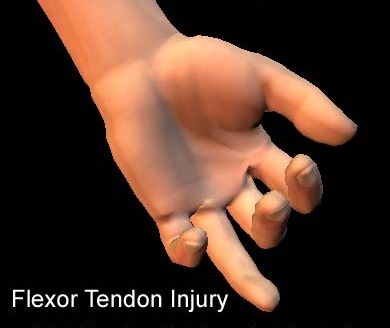
Tendon injury
Tendon injuries often present with loss of function distal to the region of injury. Few cases may also present with stiffness of distal joints owinng to non usage.
Management is primarily surgical after initial physiotherapy to attain complete passive range of motion of affected joints. Repair of tendons can be done primarily or with tendon graft or tendon transfer. This is followed with supportive medicines, splintage and physiotherapy. Physiotherapy is very crucial post surgery and starts soon after surgery and lasts for 12 weeks to 6 months depending on nature of tendon injured.

Hand Injury
Hand injury comprises a whole gamut of injuries ranging from vascular injuries to nerve injuries to tendon injuries to injuries of skin and soft tissue. Managment constitutes a thorough clinical examination followed by meticulous microsurgical surgery to restore functionality and aesthetics of the affected region.
Management varies widely based on time of presentation of patient following injury. immediate presentations are dealt with best by primary repair and reconstruction. Late/ delayed presentations are often dealt best with secondary repair ( one stage/multi stage ).

Congenital hand deformities
A congenital hand is often thought of as a functional triumph and a cosmetic disaster. It need not be so always. With availability of world class techniques many congenital hand problems like Syndactyly, Polydactyly, Congenital constriction bands can be managed with excellent functional and cosmetic outcomes. Barring circumferential constriction bands which constitute an emergency, other procedures are often done after child reaches one year of age. Splintage and physiotherapy are often needed after surgrey in this group of patients.
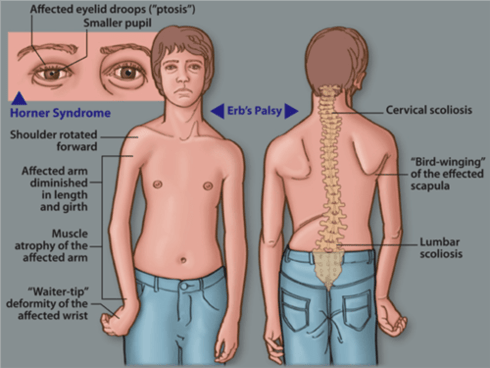
Brachial Plexus Injuries
Brachial Plexus injuries often present as complete loss of sensation and motor function of entirety or part of affected upper limb. Few cases may progress from complete to partial involvement.
Initial management is medical and supportive with usage of anti inflammatory medicines and splintage. As with other nerve injuries, this usually resolves most of the lesions. If symptoms persist beyond 12 weeks, multiple staged surgeries are a rule rather than exception. First surgery is usually exploration of the brachial plexus with nerve repair or nerve transfer ( with or without nerve grafts ) which gives better results. Secondary surgeries often involve muscle transfers (Direct / Free microvascular transfer). Splintage is almost always needed in Brachial Plexus Injuries
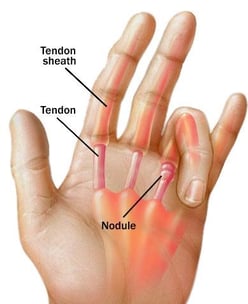
Trigger Finger
Often noticed as a jerky or snappy opening of finger, this condition may also present as fixed flexion deformity. Surgical release is definitive and gives excellent results virtually instantaneously. ( If minimal invasive manoeuvres prove unsuccessful )
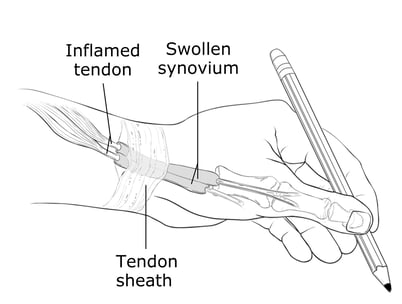
Dequervain's Tenosynovitis
Also called as De quervain's Tendinosis or Blackberry thumb. Most cases respond to conservative management with splintage and antiinflammatory medicines. If pain over thumb side of wrist persists beyond 6 to 12 weeks surgical release of tendon sheath compressing the tendons gives definitive result with near instantaneous recovery from pain and discomfort.
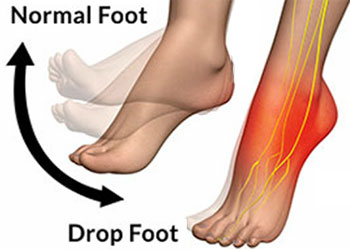
Foot drop / Common Peroneal (fibular) Nerve palsy
Often seen secondary to Knee dislocation or direct injury to Fibula or Knee surgery . As with other closed nerve injuries most cases respond to conservative management with splintage and anti-inflammatory medicines. Symptoms persisting beyond 6 to 12 weeks warrant neurolysis / nerve reconstruction most often along with a tendon transfer procedure. Surgery is followed with 12 weeks physiotherapy to retrain the rerouted tendon.

Post Injection nerve palsy / Paralysis
Inadvertent intramuscular injections into arm or Gluteal region tends to result in wrist drop and foot drop respectively. Few cases respond to conservative management with splintage and anti-inflammatory medicines. If symptoms persist beyond 6 to 12 weeks microsurgical nerve decompression and neurolysis is essential along with tendon transfer in most cases. Physiotherapy for 3 months is essential following tendon transfer
Facial Palsy
Most cases of facial palsy recover completely with medical care. In few cases with residual lesions, microsurgical reconstructive procedures aid in closure / opening of eyelids, correction of deviation of angle of mouth using nerve transfer (CFNG / Cross Face Nerve Graft) or tendon transfer ( Temporalis transfer ). Placement of gold weight in upper eyelid aids in cases of lagopthalmos.